Can Tight Hip Flexors Cause Knee Pain?
Yes, tight hip flexors, including your iliopsoas, rectus femoris, and tensor fasciae latae (TFL), can contribute significantly to knee pain, particularly pain on the outside (lateral) part of your knee. When these muscles at the front and side of your hip become tight, they create a chain reaction of biomechanical problems: anterior pelvic tilt, altered thigh position, increased stress on your IT band, and ultimately, knee pain that disrupts your training and daily activities.
However, recent research has fundamentally changed how we understand hip flexor-related knee pain. A 2024 systematic review on iliotibial band syndrome found that the problem isn't actually IT band "tightness"—it's hip muscle weakness causing poor movement patterns. The solution isn't aggressive stretching of the IT band itself, but rather strengthening the hip muscles that have failed to do their job.
Understanding Your Hip Flexors and IT Band
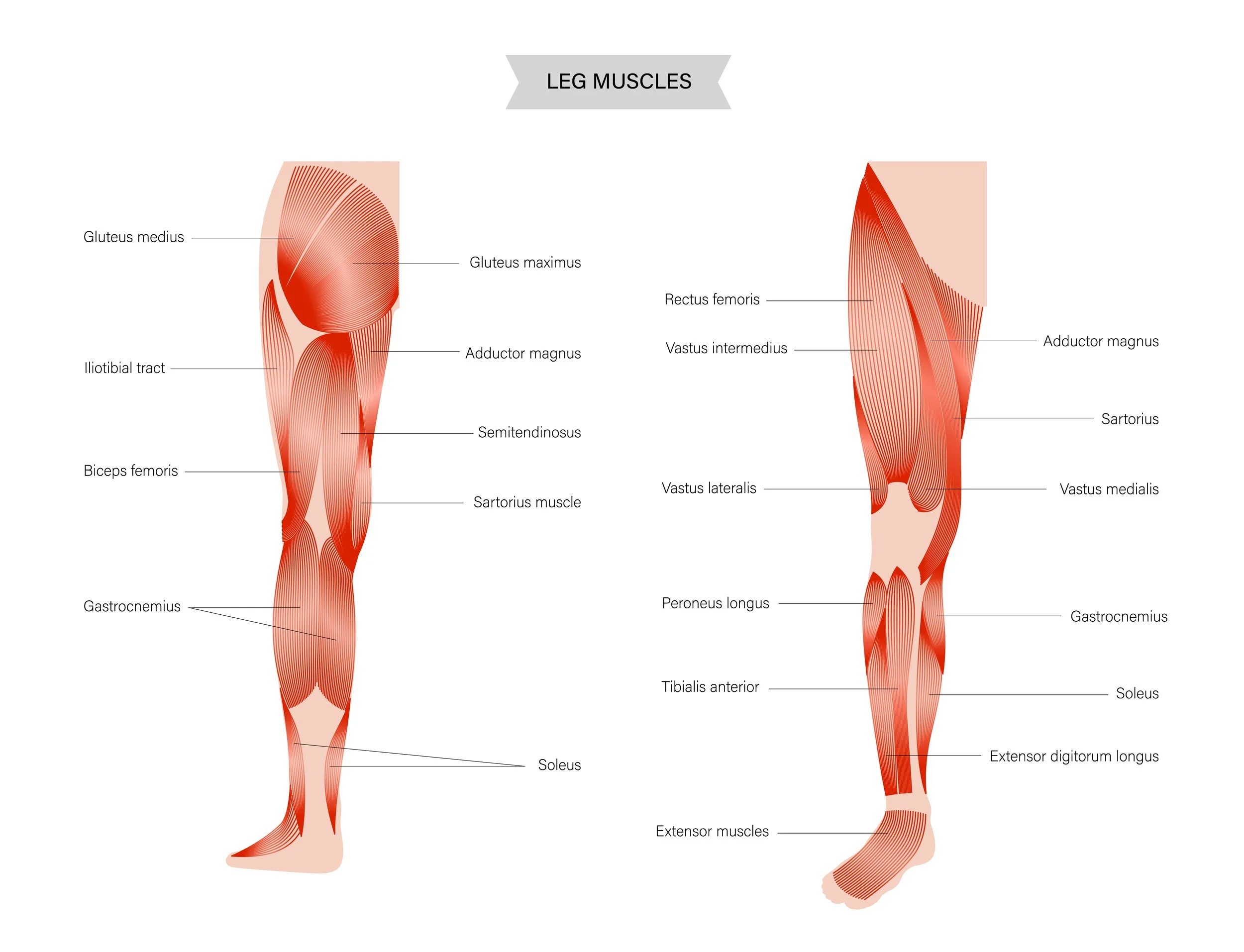
Your hip flexor complex includes several muscles that lift your thigh toward your chest:
Iliopsoas: The deep hip flexor connecting your spine to your thigh.
Rectus femoris: Part of your quadriceps that crosses both hip and knee.
Tensor fasciae latae (TFL): A small muscle on the outer hip that connects to the IT band.
The iliotibial band (IT band) is a thick fascial structure running down the outside of your thigh from your hip to just below your knee. It is fed by both the TFL and part of your gluteus maximus muscle. The IT band does not stretch, it is incredibly stiff fascia that provides stability to your leg during movement.
When your hip flexors function properly, they work in balance with your glutes and hip abductors. When they become tight and overactive, they create problems throughout your lower body, including your knees.
What Happens When Your Hip Flexors Are Tight?
Hip flexor tightness affects your knees through several interconnected mechanisms.
Anterior Pelvic Tilt and Altered Knee Loading
Tight hip flexors pull your pelvis forward into an anterior tilt. This changes the angle at which your thigh bone sits in the hip socket, which affects how forces enter your knee. The altered pelvic position increases stress on your low back and changes the Q-angle (the angle between your hip and knee), potentially increasing lateral stress on your kneecap.
TFL Overactivity and IT Band Tension
When your gluteus medius is weak, your TFL compensates by working overtime. Since TFL inserts into the IT band, this overactivity increases tension along the entire band. Recent research shows that IT band syndrome is not caused by the band being "tight", it is caused by repetitive compression of tissues beneath the band when hip muscles cannot control thigh position properly.
A 2021 systematic review in the Journal of Athletic Training found that hip abductor weakness is the primary driver of IT band syndrome, not IT band tightness itself. The compression happens at approximately 20-30 degrees of knee flexion during running and cycling when the hip drops and the thigh angles inward.
Dynamic Knee Valgus During Activity
Tight hip flexors often coexist with weak hip abductors. This combination allows your knee to collapse inward during running, squatting, and landing. The inward collapse (dynamic knee valgus) increases stress on your kneecap, overloads the inner knee structures, and creates excessive lateral pull through the IT band.
Limited Hip Extension During Gait
When hip flexors are tight, you cannot fully extend your hip during the push-off phase of walking or running. This limitation forces compensations: your low back hyperextends, your glutes cannot activate fully, and your knee absorbs more stress with each step. Over time, this altered gait pattern contributes to anterior knee pain and IT band irritation.
Rectus Femoris Compression on the Kneecap
The rectus femoris, one of your hip flexors, attaches directly to the top of your kneecap. When it is chronically tight, it creates constant downward pressure on your kneecap, compressing the cartilage underneath and contributing to patellofemoral pain.
The Updated Science on IT Band Syndrome
Recent research has fundamentally revised our understanding of IT band syndrome, with important implications for treatment.
From Friction to Impingement
The traditional model believed the IT band "rolled over" the outer part of your knee, creating friction. We now know this is wrong. Cadaver studies confirm the IT band has multiple fibrous connections to your thigh bone that prevent it from rolling.12 The pain comes from compression of a fat pad beneath the IT band, not from friction.
A 2021 review in the Journal of Athletic Training synthesized current evidence and found that strain rate (how quickly the IT band is loaded) matters more than absolute tightness. Runners with IT band syndrome show greater IT band strain throughout the support phase of running, with peak strain occurring at 20-30 degrees of knee flexion, the "impingement zone."
Hip Weakness Is the Primary Problem
Multiple studies from 2020-2024 confirm that hip abductor weakness, not IT band tightness, drives lateral knee pain. A 2020 pilot randomized trial in the Journal of Orthopaedic Surgery and Research compared IT band stretching versus progressive hip strengthening in female runners with chronic IT band syndrome. The progressive strengthening group improved on 13 outcome measures versus only 5 for stretching.
Research by Fredericson showed that 22 of 24 athletes (91.7%) with IT band syndrome returned to running after a 6-week hip abduction strengthening program, with hip strength increases of 35-50%.
The IT Band Cannot Be Meaningfully Stretched
A mathematical biomechanical model published in 2008 calculated that stretching the IT band would require forces of approximately 2,000 pounds, far beyond what any human could generate through stretching exercises. When you feel a stretch along your outer thigh, you are stretching muscles (TFL, glutes) that attach to the IT band, not the band itself.
How Do Hip Flexors and TFL Become Tight?
Several factors contribute to hip flexor tightness in active adults:
Prolonged Sitting
Hours sitting at a desk, in a car, or on the couch keeps your hip flexors in a shortened position. This chronic positioning reduces their flexibility and can lead to adaptive shortening over time.
Single-Plane Training
Runners and cyclists move primarily in a forward direction, repeatedly using hip flexion while neglecting lateral and rotational movements. This creates imbalances where hip flexors become strong and tight while hip abductors become weak.
TFL Compensation for Weak Glutes
When the gluteus medius is weak, TFL compensates during single-leg activities. This chronic overuse leads to TFL tightness and increased IT band tension, but the root problem is weak glutes, not tight TFL.
Training Errors
Rapidly increasing running mileage, adding excessive hill work, running on banked surfaces (like road shoulders), and training through pain all contribute to IT band syndrome development. Research shows approximately 60% of IT band syndrome cases stem from training errors.
Anatomical Factors
Greater-than-normal hip adduction (more common in females), internal tibial torsion, excessive foot pronation, and leg length discrepancies all increase risk for IT band issues by altering mechanics and increasing tissue strain.
How Physical Therapy Addresses Hip Flexor Dysfunction and IT Band Pain
At Victory Performance and Physical Therapy in Culver City, we follow evidence-based protocols that address the true cause of your lateral knee pain: hip muscle weakness and movement pattern dysfunction.
Phase 1: Calming the Acute Flare (Weeks 1-2)
When pain is acute, we focus on reducing inflammation and stress:
Activity modification (avoiding aggravating movements).
Ice application (15-20 minutes, 2-3 times daily).
Cross-training (swimming, stationary cycling with bike fit adjustment).
Low-load hip activation exercises.
Gentle manual therapy to tight muscles.
Not recommended: Deep friction massage to IT band, aggressive IT band stretching, or corticosteroid injections (evidence shows limited benefit).
Phase 2: Building Hip Strength (Weeks 2-6)
The core of effective treatment focuses on hip abductor strengthening:
Side-lying hip abduction (3 sets x 15-30 reps).
Clamshells with progressive resistance.
Single-leg hip hikes (preventing pelvic drop).
Standing hip abduction with bands.
Side planks for hip stabilizer endurance.
Research supports high-quality movement with eccentric control focus. We progress resistance from band at knees to ankles to forefeet, with studies showing forefoot band placement provides optimal gluteal activation.
Phase 3: Functional Loading (Weeks 4-8)
We progress to weight-bearing exercises that challenge your hip control:
Single-leg stance exercises.
Forward and lateral lunges.
Step-ups and step-downs (4-8 inch platform progressing higher).
Lateral band walks.
Single-leg mini squats (preventing knee valgus).
Progression criteria include pain 3/10, high-quality sagittal plane motion, and no Trendelenburg gait pattern.
Phase 4: Return to Sport (Weeks 6-10+)
The final phase prepares you for high-demand activities:
Deep single-leg squats.
Lateral hops and bounds.
Drop jumps (bilateral single-leg progression).
Agility drills.
Run-walk intervals (starting 1:1 ratio, progressing to continuous running).
Effective Hip Flexor Stretching
While strengthening hips is primary, targeted hip flexor stretching can help:
Kneeling hip flexor stretch (pirate stretch): Targets iliopsoas and rectus femoris, 30 seconds X 3 reps, 2x daily.
TFL-specific stretch: Based on 2015 ultrasound research: hip extension + adduction + external rotation + knee flexion 90 degrees, held 30 seconds X 3-5 reps.
Dynamic hip flexor mobilizations: Performed as warm-up before activity.
Important: These stretches supplement hip strengthening but do not replace it.
Manual Therapy Adjuncts
Evidence supports manual therapy when combined with exercise:
Hip joint mobilizations (improve mobility for effective strengthening).
Soft tissue mobilization of TFL and hip flexors (reduce tension).
Neuromuscular re-education (motor control training).
Extracorporeal shockwave therapy (emerging evidence for IT band syndrome).
A 2024 systematic review found that multimodal approaches combining strengthening with manual therapy produced pain reductions of 27-100% and functional improvements of 10-57% over 2-8 weeks.
Evidence-Based Treatment Outcomes
Research consistently demonstrates strong outcomes when hip weakness is properly addressed:
IT Band Syndrome Recovery Rates:
Mild cases: 100 percent recovered in 2 to 4 weeks
Average cases: 100 percent recovered in 7 to 8 weeks
Severe cases: 100 percent recovered in 9 to 24 weeks
Effectiveness of Hip Strengthening:
91.7 percent of athletes return to running after 6-week hip abduction program
Hip strength increases of 35 to 50 percent
Pain reductions of 27 to 100 percent
Functional improvements of 10 to 57 percent
Long-Term Outcomes: Studies show 50 to 90 percent improvement with conservative treatment in 4 to 8 weeks, with good prognosis following proper management emphasizing hip strengthening and biomechanical correction.
What Doesn't Work for IT Band Pain
Based on current evidence, several traditional approaches lack support:
Not Effective or Not Recommended:
Aggressive IT band stretching (can't meaningfully lengthen fascia)
Deep friction massage to IT band (limited evidence, no proven benefit)
Foam rolling IT band (may provide temporary relief via mechanoreceptor stimulation but doesn't address root cause)
Corticosteroid injections beyond 2 weeks (limited long-term benefit)
Continuing high-volume training without addressing hip weakness
The Ober Test Misconception: Research from 2016 showed the Ober test is not valid for measuring IT band tightness. A positive test indicates hip muscle tightness, not IT band restriction.
Why Hip Strengthening Works When Stretching Doesn't
Many runners and athletes spend months stretching their IT band and hip flexors without improvement because they are not addressing the root problem—hip muscle weakness that allows poor movement mechanics.
When you strengthen your hip abductors and correct movement patterns:
Your pelvis stays level during single-leg stance.
Your thigh stays aligned instead of rotating inward.
Forces distribute more evenly through your knee.
IT band strain decreases naturally without stretching.
You build resilience against future flare-ups.
You are fixing the mechanical dysfunction, not just chasing symptoms.
Comprehensive Care at Victory Performance and Physical Therapy
At Victory, we recognize that hip flexor and IT band issues require comprehensive assessment and treatment. We evaluate:
Hip abductor and gluteus medius strength
TFL tension and overactivity patterns
Hip flexor flexibility and strength
Movement quality during squatting, lunging, and single-leg stance
Running mechanics (stride rate, hip drop, knee valgus)
Training load and volume
Your personalized treatment plan addresses all factors contributing to your lateral knee pain, not just one piece of the puzzle.
What to Expect From Treatment
Most active adults see significant improvement in 6 to 8 weeks with proper hip strengthening protocols.
Success indicators include:
Hip abductor strength improvements of 35 to 50 percent
Symmetry between injured and non-injured sides
Pain reduction during running and functional activities
Single-leg squat quality (no knee valgus or Trendelenburg)
Progressive return to full training volume
The timeline depends on symptom duration, training demands, and adherence to exercise programs. Acute cases (less than 3 months) typically improve in 4 to 8 weeks, while chronic cases (greater than 3 months) may require 8 to 12 weeks.
Take Control of Your Lateral Knee Pain
Tight hip flexors and IT band pain do not respond to stretching alone because the real problem is hip muscle weakness allowing poor mechanics. But targeted physical therapy that strengthens your hips, corrects movement patterns, and manages training load can resolve even chronic lateral knee pain.
At Victory Performance and Physical Therapy in Culver City, we use evidence-based protocols that address the root cause of IT band syndrome and hip flexor-related knee pain. Whether you are a runner dealing with persistent lateral knee pain, a cyclist fighting IT band issues, or an athlete limited by hip and knee dysfunction, our team can help.
Don't waste more time on treatments that do not address the real problem. Schedule an evaluation today with our expert physical therapists and discover how hip strengthening can eliminate your knee pain for good.
📅 Call Today: 424-543-4336